
The natural, Functional Medicine approach to fertility success
First up: if you’re reading this, you may want to head over to our new dedicated Coho Fertility website where you’ll find this article, and lots more fertility related goodness!
Fertility issues in men and women are on the rise globally.
This trend is, unfortunately predicted to continue.
At the time of writing, an estimated 8-12% of couples are having difficulty conceiving and sadly, around 10-15% of pregnancies end in miscarriage.
The Functional Medicine approach to fertility

We know that the emotional (as well as the financial) investment in a fertility journey can be painful and not knowing where to turn to next, extremely confusing.
What is often missing, is a thorough, root-cause, systems-based approach.
A functional medicine approach to fertility that leaves no stone unturned in
identifying possible imbalances that are hindering pregnancy, and then addressing these imbalances.
Table of Contents
We work with men and women, whatever the situation may be – whether you’re:
- Trying for a natural conception
- On an IVF or other assisted treatment journey
- Looking at surrogacy
- Or using an egg and/or sperm donor
- Have suffered multiple IVF round failures
- Have suffered miscarriages
The Coho Functional Medicine approach to fertility is to identify all of the underlying imbalances that may be contributing to fertility issues.
We do this through extensive screening questionnaires, through listening to you, and through selecting the most appropriate testing for your issues.
We then address these through an evidence-based, integrative approach which is 100% tailored to each individual given individual findings, personal circumstances, test results, genetic pre-dispositions, family history, signs and symptoms.
Apply for your free 15 minute Discovery Call with Dee Brereton-Patel now
Our extremely high success rate – even with those who have suffered multiple failed rounds of IVF and / or have suffered repeated miscarriages, is based on our in-depth, functional medicine approach to fertility.
We understand that a fertility journey can be heart-breaking and life-changing.
We passionately believe that you should be aware of all of your options, and have the opportunity to dig deeper into your fertility, gain greater understanding of what might be holding your fertility back, and have the tools to do something about it.
Infertility statistics
An estimated 48 million couples, and 186 million individuals worldwide live with infertility and the fertility rate has halved in the past 50 years.
Around 50% of all cases of infertility are due to female factors alone, 20-30% are due to male factors alone, and the remaining 20-30% are due to a combination of male and female factors (1).
This means that in at least 40% of cases, there is a fertility related issue in the male partner.
This is an important fact – the fertility investigative process should be performed by both the female and male partner.
All too often however, it can be the female that is left carrying the majority of the burden on the fertility journey.
Guys, many of you need to up your fertility game!
In same sex couples or single mums-to-be, the scenarios will be different, but essentially the health of the egg, the sperm, and the person carrying the pregnancy, all need to be considered to optimise the chances of success.
This is where a functional medicine approach to fertility can help to achieve great success.

Dee was recommended by a friend and I didn't hesitate to contact her.
She helped to track any single problem that could prevent a pregnancy by running some tests and then recommended supplements and diet that helped.
When GP was only talking about my problems, Dee was looking at both and made sure we were both healthy.
We were so thrilled to find out that we were expecting which wasn't the end actually. We continued working together through my whole pregnancy, making sure I take all the necessary vitamins for my body to be able carry a healthy baby.
Healthy mama, healthy baby!
I had such an easy pregnancy (I kept telling Dee, that I don't feel pregnant at all :))) and no postpartum issues.
All my friends warned me to be ready for falling hair, gum diseases etc. but I had non of that and I know it's because my body wasn't deficient of any vitamin or mineral.
I am super proud to say that now I am a mum of beautiful baby boy.
Knowing that Dee and her team exist gives me a comfort as I know that if we ever have some health issues in the future (touch wood), I'll contact them straight away.
Fertility success starts with a proper analysis
In our experience we find that men and women seeking a systems biology, Functional Medicine approach to fertility, have not yet received a thorough investigation.
A semen analysis may have been performed for the man, and possibly some basic hormonal tests for the woman (the day 21 progesterone test, LH, FSH, oestradiol, AMH).
Perhaps more advanced testing has been performed, such as NK cells, scans, HyCoSy (Hysterosalpingo Contrast Sonography) or autoimmune testing.
And that’s even in complex cases, and cases where there are persistent fertility issues.
Our view: based on our years of experience with fertility clients, this level of analysis is absolutely inadequate, and is not capable of identifying the root causes that underpin many fertility issues.
Our experience suggests it’s usually the case that ‘some’ work-up has been done, but some critical understanding of underlying factors, is yet to be in place.
And if by chance you’re reading this and have been diagnosed with ‘unexplained fertility‘, please do stay with us for a little while longer and keep reading…
Infertility: the male factor
Let’s take a second to give a shout out to our equally important male partners out there…
Guys – getting on board is non-negotiable.
At Coho we have been lucky enough to work with amazing men who are totally on this journey with their partner.
Unfortunately in our experience, there are also a good number of men out there who see the fertility journey as a ‘female only’ responsibility, refusing to make the necessary nutrition and lifestyle changes while their partner is left to make up the ground.
We’ve even seen some who refuse to take a supplement.
So we have to be clear, if you’re in the 40% of infertility cases where the male is playing a role in that fertility, you need to get in the game.
The male involvement does not stop with the provision of one healthy looking sperm (as we discuss further below).
Infertility: root cause factors
It all sounds simple right?
So why can it be so difficult for some people to conceive and maintain a healthy pregnancy?
Lets take a dive into the root cause factors that could be contributing to fertility issues (please note that this is not an exhaustive list but in our experience, are the most common factors);

Structural issues in fertility
In some cases, knowing whether structural factors are at play (e.g. blocked fallopian tubes or testicular problems) is impossible to know unless the right investigations are performed.
If you’ve been trying to get pregnant for some time and it’s just not happening, consider requesting some scans and tests through your doctor to check for any structural abnormalities in the female and male reproductive system.
Often any issues can be corrected through simple surgical procedures.
This can be THE barrier to pregnancy and is important to understand.
Female structural abnormalities
Blocked fallopian tubes can stop the sperm cell from travelling to through the fallopian tube in the female, where it can meet with and fertilise an egg.

A Hysterosalpingo Contrast Sonography (HyCoSy) is an ultrasound technique used to check the uterus and fallopian tubes.
The uterine cavity can be assessed through a 3D ultrasound scan, checking for any abnormalities that could be affecting implantation.
A thin tube (catheter) is inserted through the cervix, that then carries a dye (contrast material) which is tracked on an ultrasound scan.
If the dye travels all the way through the tubes into the uterus, then this confirms that the tubes are open.
If the dye is not travelling through into the uterus, then this indicates a blockage.
This can be a complete blockage, or a partial blockage, affecting just one fallopian tube or affecting both.
If there is any sign of tubal obstruction or damage then this may be further investigated with a laparoscopy or hysteroscopy.
Couples may be trying to conceive naturally, but not achieving a positive pregnancy test due to lack of fertilisation of the egg with the sperm, simply because they are not able to meet.
Assisted reproductive procedures can help with bypassing the fallopian tubes, or surgery can be an option in some cases to remove the blockage.
Causes of fallopian tube damage or blockage include endometriosis, infection or pelvic inflammatory disease (2,3).
Congenital abnormalities
Some women are born with uterine abnormalities (congenital), including a double uterus (bicornuate), uterine septum, and a uterus in which only one side has formed (unicornuate).
In many cases, an abnormally shaped or positioned uterus is not likely to prevent fertilisation, but can interfere with normal embryo implantation (4).
Ultrasound scans can be helpful in providing further information.
It’s possible to have such issues, but carry a normal pregnancy, as the abnormality hasn’t affected implantation or blood supply to the foetus, or caused any obstructions as baby grows.
Some structural abnormalities can be corrected with surgery.
Studies have estimated that the prevalence of congenital uterine abnormalities is around 16% in women with recurrent miscarriages, and 7.3% in infertility (5).
PCOS (Polycystic Ovary Syndrome)
PCOS is a leading cause of infertility in women.
Some women with this condition have pearl-sized cysts or follicles that can be seen on ultrasound scans.
Eggs from the ovaries are released each month during the ovulation phase of the menstrual cycle.
The eggs are in tiny sacs called follicles that fill up with fluid as the eggs mature.
Each cycle, the most mature follicle breaks open to release a mature egg which may be fertilised.
Due to hormonal changes that occur in women with PCOS, the eggs do not fully mature.

The follicles grow and build up fluid, but the follicles don’t rupture and release the egg(s), and so there in no ovulation.
The follicles then become dormant and are seen as cysts on a scan.

Not all PCOS cases have ‘cysts’, some cases of PCOS are diagnosed based on other criteria (such as high androgens and irregular menstrual cycles) (6).
Endometriosis
Endometriosis can influence fertility in several ways, and is present in 25 to 50% of women with infertility (7).
From a structural perspective, the endometrial tissue can affect the uterine cavity or affect the fallopian tubes or ovaries.
Scans can show if the endometrial tissue is being obstructive to normal fertility processes, including if the tissue is likely to get in the way of embryo implantation.
There are other mechanisms in endometriosis that can affect fertility that we’ll come to shortly (such as hormonal changes and increased inflammatory cytokines) (8).
Fibroids
Fibroids affect around 5-10% of women with infertility (9).
Fibroids are muscle tissue (non cancerous) that change the shape or size of the uterus and sometimes the cervix.
Whether fibroids cause symptoms or require treatment depends on their location, size, and number.
Fibroids that affect the interior of the uterus can affect implantation and pregnancy loss risk.
A Functional Medicine approach to fertility, and in fibroids and endometriosis can:
- help to reduce the underlying drivers of these conditions
- improve the hormonal imbalances that often exist in these conditions
- and improve the non-structural consequences such as inflammation
Inflammation, no matter what the cause, can adversely affect fertility, in both men and women (10).

Male structural abnormalities affecting fertility
A physical examination (or scan) can reveal if there are any structural abnormalities in the male genital area.
Varicoceles
The most common structural finding in male infertility, are varicoceles (11).
A varicocele is an enlargement of the vein that transports oxygen-depleted blood away from the testicle.
These veins are on the scrotum (that hold the testicles).
The dilated veins increase the temperature to the testicular area, where the sperm cells are produced.
Sperm cells are very sensitive to changes in their environment – changes such as increased temperature, pressure, or oxidative stress (12).
The increase in temperature is believed to damage DNA in the cells that produce sperm.
This leads to sperm abnormalities such as decreased sperm count or motility, as well as increased DNA damage (increased DNA fragmentation (13) – something we test for, in our male clients).
Retrograde ejaculation
Retrograde ejaculation occurs when the neck of the male bladder fails to close during orgasm, causing semen to move back into the bladder, rather than out through the penis.
It is possible to not notice retrograde ejaculation.
Other symptoms that are more noticable are:
- if little or no semen is produced
- urine after an orgasm is cloudy
- or fertility issues
Retrograde ejaculation results in low sperm count (14) and may be caused by:
- prior surgery to the prostate
- diabetes
- medications taken for high blood pressure
- depression
The tubes where sperm are produced in the testes (vas deferens) and where sperm are stored (epididymis) can be affected by infections, surgeries or genetic conditions, and in some cases can lead to obstructions that halt sperm delivery.
Obstructions in these tubes that deliver sperm cells can affect sperm count.
Around 4-10% of men with low or no sperm count may have an obstruction.
Female Hormonal Imbalances
Clinical guidelines state that the median menstrual cycle length is 28 days.
Many tests and scans are based on this assumption that the ‘normal’ cycle length is 28 days. The menstrual cycle is dependant on a number of hormones.
Chief among these hormones are:
- oestrogen
- progesterone
- luteinising hormone (LH)
- follicle-stimulating hormone (FSH)

However, the ideal, 28 day menstrual cycle often does not exist.
A cycle that is slightly shorter or longer, between 25-30 days long and is the same length each cycle, is also considered normal.
Our clients often have extended menstrual cycles (for instance a 35 day cycle instead of a 28 day cycle), infrequent cycles, or the complete absence of a cycle.
One of the most common early infertility related female hormone checks performed, is the Day 21 Progesterone test.
Progesterone is checked on day 21 as it’s considered the day when progesterone levels should be at its highest during a menstrual cycle, based on a 28 day cycle.
We’ll talk in a second about why this test can be flawed.
High levels of progesterone confirm ovulation, and that the corpus luteum (tissue formed from the leftover follicle after ovulation) is producing progesterone (15) to support egg implantation and pregnancy.
If there is a low progesterone result in a cycle, then the test should be repeated in a new menstrual cycle before any conclusion is made.
It is possible that the ‘Day 21’ progesterone is low in one cycle, but normal in the next cycle.
More helpful is regular progesterone testing over the course of a full cycle, rather than relying on a single (one time point) progesterone test.
However, if your cycle length is ‘not’ 28 days, then the test day needs to be adjusted.
Otherwise, collecting a sample on day 21 could mean that you miss that peak level you’re looking for.
For example, in a 31 day cycle, you’re better off doing the ‘Day 21’ progesterone test on day 24.

The peak progesterone level also depends on when ovulation occurs.
This isn’t exactly on the same day, every cycle, for every woman.
Another factor to bear in mind is that in irregular cycles, a woman might not know when she is ovulating and therefore when to expect the mid-luteal phase peak.
Lastly, progesterone is released in pulses (16) and a blood sample at 9am may show low levels of the hormone, but a sample 4 hours later on the same day may show a normal reading.
For all of these reasons, the Day 21 Progesterone isn’t a great tool and can cause unnecessary worry.
Better female hormone testing
At Coho Health, our go-to test for hormone analysis is the DUTCH test.
In our, natural, Functional Medicine approach to fertility, DUTCH (Dried Urine Test for Comprehensive Hormones) testing can help us to understand progesterone and oestrogen levels over the course of a whole menstrual cycle.
Wouldn’t it be great if you could see your oestrogen and progesterone levels over a full cycle?
And understand how long your follicular and luteal phases are, if you are actually ovulating, and if you are producing appropriate oestrogen and progesterone levels at the appropriate time of the month?
Taking the guess work out, and delivering accurate meaningful results is a game-changer both for practitioners and clients.
For us, it means that we know exactly what needs to be done and how we can help you optimise your fertility.
Since coming off the contraceptive pill my cycle had not regulated and I had many unanswered questions around my health.
Although I did much research myself into functional testing, supplements and lifestyle changes to assist my journey it had become a confusing minefield of options which resulted in me needing guidance.
Working with Coho Health gave me the access to functional testing not available on the NHS / without a practitioner that could give me more insight into the possible causes of my infertility.
They also interpreted the results which would be very difficult/impossible alone.
My partner also worked with a member of the Coho health team, our results combined identified issues that resulted in us having our NHS funded IVF round as an ICSI round (rather than standard IVF which would have likely failed) and I have gone on to have a successful pregnancy from this for which we are extremely grateful.
Although we didn't manage to conceive naturally which has been our original hope, we do feel that the diet and lifestyle changes plus supplements aided us in getting pregnant on our first and only NHS funded round of IVF/ICSI.
I have learnt valuable information around diet and lifestyle that I will aim to retain and continue to use going forward.
I would recommend Coho Health, Dee has been kind and supportive throughout my journey and I would recommend to anyone requiring guidance and direction on their fertility journey.
Thanks Coho Health
Oestrogen testing & oestrogen dominance in fertility

If oestrogen levels are higher, then this is considered to be oestrogen dominance.
In oestrogen dominance, the oestrogen level could be normal.
But when progesterone is low, then when you compare oestrogen to progesterone, the oestrogen is still higher even though the level in the test shows as normal.

Oestrogen dominance increases the risk of infertility and pregnancy loss (17).
Other symptoms of oestrogen dominance include:
- short luteal phase
- heavy bleeding and clotting
- fibrocystic breasts
- headaches
- brain fog
- fatigue
- poor memory
- miscarriage
Conditions associated with oestrogen dominance include:
- fibroids
- fatigue
- poor memory
- miscarriage
High oestrogen
Oestrogen levels can be higher than optimal due to:
- increased hormone production
- increased exposure to xenoestrogens (environmental molecules that mimic oestrogen in the body, such as plastics or hormones in non-organic meat)
- or decreased oestrogen detoxification
It can be helpful to break down how we view oestrogen in the body into three stages:
1/ we make oestrogen
2/ then we use oestrogen
3/ and then we need to clear (detoxify and eliminate) oestrogen

To ‘clear’ the ‘old, ‘used’, oestrogens, we need good liver function (phase 1 enzymes and phase 2 detoxification pathways – glucuronidation and methylation) and normal stool frequency (constipation can exacerbate the issue).
Gut testing and oestrogen elimination
Functional tests assessing gastrointestinal function, often include an enzyme called beta-glucuronidase which we find very useful.
It’s an enzyme that, at high levels, slows down the elimination of ‘used’ oestrogen through the bowel (18).
Gut bacteria imbalances (dysbiosis) and lack of certain nutrients, can increase beta-glucuronidase, and an optimal microbiome and nutrient status can reduce levels.
Adrenal Stress Hormones
In the Coho Functional Medicine approach to fertility, our experience is that adrenal (stress) hormone imbalances are THE most common factor that reduces fertility.
We’ve seen it with our fertility clients on many, many occasions.
When stress is reduced and is better managed, then fertility is improved.
Why?
Stress is so intricately connected to many other systems and functions in the body.
Stress hormone imbalances affect the thyroid hormones, pituitary hormones, the circadian rhythm, melatonin levels, sex hormone levels, sperm and egg quality.
Stress comes from many different sources; emotional, mental, physical, poor immune system, low mood, low thyroid, hidden food sensitivities, inflammation, infections, blood sugar dysregulation, poor sleep and environmental toxins.
So even if we don’t ‘feel’ stressed, it may be that physiologically, the body is having a response to one or more stressors.
All of these different ‘stressors’ impact our stress hormones (of particular importance are cortisol and DHEA levels).
In men and women, stress can suppress Luteinising Hormone (LH). In men, low LH can cause low testosterone and low sperm cell production (19).
In women, low LH can prevent ovulation, cause low progesterone levels, and increase miscarriage risk (20).
Studies have shown that psychological stress changes semen parameters (reduced sperm concentration, motility and morphology) (21).
Research has also shown that stress management techniques improve outcomes in assisted reproductive treatment (22).
An invaluable testing option available to us, and which we run for almost all of our clients who are struggling with their fertility, is the comprehensive DUTCH hormone tests by Precision Analytical.
It is absolutely the best way to understand hormones and how they are connected to each other, and how the body is breaking down and clearing hormones.
There are different options in performing the DUTCH hormone tests.
For females, dried urine samples are taken at specific time points throughout the cycle (when performing the DUTCH Cycle Mapping test).
Or several samples at are collected at specific time points in the mid-luteal phase of the cycle (if performing the DUTCH Complete or the DUTCH Plus tests).
The DUTCH tests include a thorough assessment of:
- cortisol, and DHEA (our ‘stress hormones’)
- DHEA-S
- testosterone (and other androgens)
- progesterone (and its metabolites)
- oestrogen (oestradiol, oestrone and oestriol)
- and oestrogen metabolites (the end products of oestrogen metabolism before they are eliminated from the body)
Seeing the stress hormones with the sex hormones in the same report can help us to understand the impact stress may be having on fertility.
Once we have this detailed information, stress hormones can be modulated in different ways, depending on what the individual presentation is.
Some strategies we would consider in a functional medicine approach to fertility include:
- helping our clients establish regular sleep-wake cycles
- implementing regular stress reduction activities
- appropriate exercise at the appropriate time of day (guided by the cortisol results over a 24 hour period)
- balancing blood sugar levels through nutrition and meal timings
- adrenal supportive nutrients or herbs such as those listed below
Apply for your free 15 minute Discovery Call with Dee Brereton-Patel now
Please note that in our Functional Medicine approach to fertility, supplements are specifically recommended to each of our clients based on their individual results and symptoms.
All of the below nutrients/herbs are not appropriate in every case as they have different mechanisms of action:
- magnesium
- vitamin C
- vitamin B5
- vitamin B6
- ashwagandha
- rhodiola
- ginseng
- reishi
- phosphatidylserine
- cordyceps
- bacopa monnieri
Low thyroid hormones (hypothyroidism) & female fertility
When it comes to fertility and infertility, thyroid hormones should be evaluated for everyone.
Thyroid hormones secreted from the thyroid gland (which sits just below the voice box) are important signals to the ovaries and endometrial tissue, playing a critical role in fertility.
Thyroid hormones can affect menstrual cycle length (about half of hypothyroid patients have menstrual irregularities), can support ovulation, help to maintain a fertilised egg, support implantation and reduce the risk of early pregnancy loss.
The regulation of the reproductive system is perhaps one of the most relevant actions of thyroid hormones.
Hypothyroidism (or sub-clinical hypothyroidism), i.e., low thyroid hormones, is much more common than hyperthyroidism (increased thyroid hormone levels).
Low thyroid hormones in females affects:
- ovulation
- shortens the luteal phase of the menstrual cycle
- causes light or heavy periods
- increases pregnancy loss
- and affects the functioning of the endometrium and placenta (causing implantation issues and increasing pregnancy loss risk)
Research clearly points to an optimal TSH of 2.5 or less to support fertility and reduce pregnancy loss risk (23, 24).
Fertility clinics we’ve worked with are also using the same range for TSH.
But unfortunately, in tests performed at fertility clinics, even though they are using the same range, we do often see TSH levels higher than 2.5 that have not been flagged as a concern for fertility.
As TSH levels can slightly fluctuate, and in pregnancy it is natural for the TSH to rise, in our functional medicine approach to fertility, we aim for clients to have a slightly lower TSH to compensate for these factors.
Therefore, we work with clients to achieve a TSH of no higher than 2.
Optimal upper end of TSH range for fertility in clinical practice is 2
It is possible to feel ‘no’ symptoms of thyroid imbalances, but still have thyroid hormones in the sub-clinical range (where the tests that your doctor performs, would fall within the ‘normal’ range)
Sub-clinical thyroid hormone levels can affect fertility (25).
Thyroid hormones are also key to reducing pregnancy related risk factors for the mother, as well as affecting birth outcomes.
Comprehensive thyroid hormone testing is a must for everyone who is struggling with fertility or who wants to ensure they are in optimal health for pregnancy.

High anti-thyroid antibodies in female fertility
Testing should always include test for thyroid antibodies (but this is hardly ever included in regular testing).
Anti-thyroid antibodies (involved in 90% of hypothyroid cases) affect fertility independently of thyroid hormones.
Elevated thyroid antibodies are a risk factor for infertility and miscarriage, even before other thyroid hormone levels are affected (26).
Whilst sufficient thyroid hormones help to achieve and maintain a pregnancy, anti-thyroid antibodies are equally as important.
And in-fact it is the circulating anti-thyroid antibodies, that are most commonly the cause of thyroid dysfunction.
Anti-thyroid antibodies are produced by the immune system, and essentially ‘attack’ healthy thyroid cells, causing dysfunction.
The most prevalent anti-thyroid antibodies are the thyroid peroxidase antibody and thyroglobulin antibody.
It is possible to have elevated thyroid antibodies without having thyroid hormone levels outside of the normal range.
And whilst mainstream medical doctors do not treat high thyroid antibodies, they are certainly a factor in fertility.
In the conventional medical model, doctors would wait until the anti-thyroid antibodies cause enough thyroid tissue destruction, that the gland starts to produce abnormal levels (usually low levels) of thyroid hormones.
It is at this stage, that doctors would intervene with levothyroxine medication (synthetic thyroid hormone, specifically T4 hormone).
However, understanding anti-thyroid antibody levels, as well as thyroid hormone levels is vital in all fertility cases.
Women may have normal thyroid hormone levels, but high anti-thyroid antibodies.
There is evidence that these antibodies can adversely affect conception and pregnancy outcomes.
Higher anti-thyroid antibodies have been correlated with (27):
- reduced egg fertilisation
- lower quality of embryos
- reduced pregnancy rates in IVF
- and increased early miscarriage rate
The antibodies may create inflammation that can damage maturing eggs (oocytes) reducing egg quality.
Anti-thyroid antibodies may also be a sign of more systemic immune system imbalances and oxidative stress that can affect ovarian reserve and embryo quality.
Oxidative stress is caused by an imbalance between the production of oxygen reactive species (ROS) in cells and tissues, and the ability for the body to ‘neutralise’ and detoxify these reactive products.
ROS levels are reduced, and the damage they cause to cells is reduced, by antioxidants.
Thyroid Peroxidase and Thyroglobulin antibodies are the main thyroid antibodies, and can be easily measured.
This is often an overlooked assessment in those with fertility issues.
Low thyroid function and / or high thyroid antibodies can negatively affect conception rate, pregnancy loss and birth outcomes.
Low thyroid hormones (hypothyroidism) & male fertility
Low thyroid hormones also impacts male fertilty.
Thyroid hormone deficiency can reduce spermatogenesis (the development of new sperm).
And can result in lower sperm count and motility, and can contribute to erectile dysfunction and low libido (28).
Pituitary hormones in fertility
When there are challenges in the fertility journey, it is common in conventional medicine for the pituitary hormones to be investigated.
With our fertility clients, we always ensure these checks are performed.
The hormones produced by the pituitary gland act as signals from the brain to the testes and ovaries.
These signals control sex hormone levels and reproductive processes.
These hormones are Luteinising Hormone (LH), Follicle-Stimulating Hormone (FSH) and prolactin.
In women, the LH surge (measured in ovulation tests) triggers the release of an egg from a follicle (ovulation), and FSH stimulates the growth of the follicles.

In men, LH signals to the testes to produce testosterone, and FSH is responsible for sperm cell synthesis (spermatogenesis).
Prolactin in fertility
Prolactin is a hormone produced by the pituitary gland that is responsible for lactation and certain breast tissue development.
Prolactin levels should be relatively low in men and women, and only increase in women after childbirth to support lactation.
Prolactin, and especially high levels of prolactin, can play an important role in fertility in both men and women.
High prolactin can result in lower FSH and LH levels, which in turn can result in irregular menstrual cycles or the absence of cycles (amenorrhea) (29).
See the section in red in the Luteinising Hormone & FSH in Women infographic above to see a visualisation of how this works.
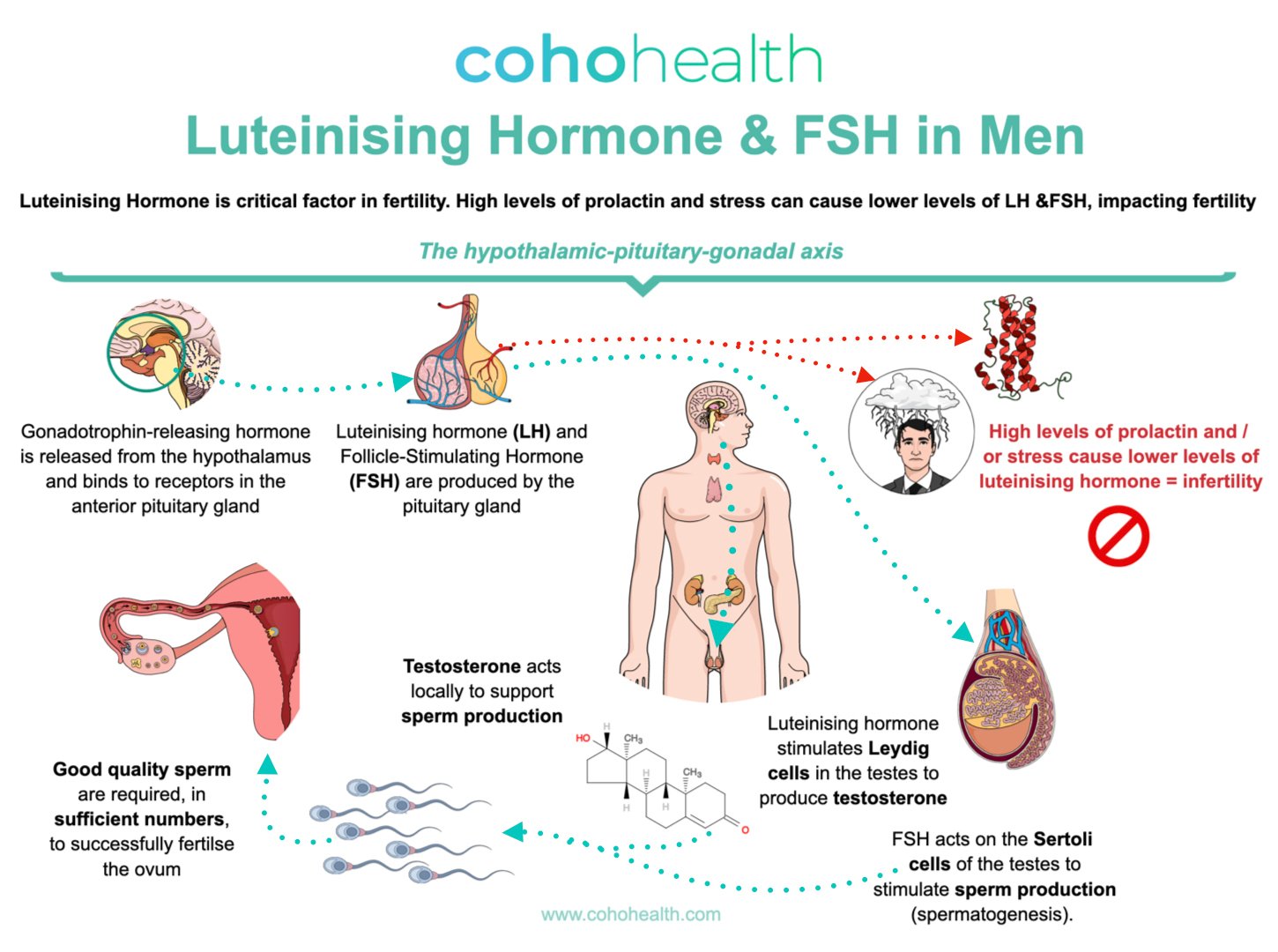
Men can also have high prolactin levels (may be prevalent in up to 11% of infertile males and is a diagnosis that is often missed) (30).
High prolactin levels in men inhibits the release of FSH and LH from the pituitary gland.
Low levels of LH and FSH cause issues in the testes, notably reduced spermatogenesis (sperm cell production) and reduced testosterone levels.
See the section in red in the Luteinising Hormone & FSH in Men infographic above to see a visualisation of how this works.
Pituitary (brain) communication with the ovaries and testes is a critical pathway, controlling reproductive hormones and functions.
Insulin in fertility
In the Coho functional medicine approach to fertility, insulin is a real problem for both men and women.
A normal level of insulin is required for our cells to utilise blood glucose.
However, when our cells stop listening so well to the circulating insulin, the pancreas makes more insulin to compensate.
This higher level of insulin then goes on to cause a state known as insulin resistance.
This isn’t necessarily the level of insulin that is seen in prediabetes or diabetes, it can be a more subtle imbalance, that plays havoc with fertility.
Insulin resistance promotes:
- inflammation (31)
- oxidative stress (32)
- metabolic syndrome (33)
- higher blood pressure (33)
- reduced sperm (34)
- reduced egg quality (35)
- higher androgen hormones (36)
- and imbalanced pituitary hormones, leading to oestrogen and progesterone imbalances (37)
So you can see that the down stream effects of insulin resistance are significant!
As we know, insulin surges in response to eating carbohydrates or sugars.
In turn, high insulin increases testosterone and DHEA levels.
Higher levels of testosterone and DHEA are common in PCOS, and insulin resistance is closely associated with PCOS.
A fasting insulin test (something which is not routinely tested) is one of the earliest indicators of an insulin problem.
A high fasting insulin result points towards reduced insulin sensitivity (this is way before someone might see a high fasting glucose, or high HbA1c result).
Insulin resistance drives infertility via several mechanisms.
The earliest indicator of a problem with insulin, is a high fasting Insulin test.
Improving insulin sensitivity
Insulin sensitivity can be improved in most cases through relatively simple nutritional and lifestyle interventions.
Some factors to consider in increasing insulin sensitivity, include;
– Reduce carbohydrate intake to help stabilise blood glucose levels and reduce the need for the body to produce high surges of insulin.
Carbohydrates come in many forms, the ‘worst’ carbohydrates in terms of insulin production turn into glucose quickly.
They include foods with refined sugars such as cakes, cookies, chocolates, ice cream, sweets, desserts and high amounts of maple syrup and honey.
Then there are flour-based products such as bread, pastry, biscuits and pizza that turn into glucose relatively quickly and provoke an insulin response.
A high amount of starchy carbohydrates such as potatoes (and potato products like chips), parsnips, squash can also raise blood sugar levels too high.
Alcohol, soft drinks, fruit juices and squash are also a problem.
– Increase fibrous vegetable intake to boost fibre and nutrient intake.
Include a variety of vegetables that grow above ground, and a range of different colours; chard, spinach, broccoli, cabbage, cauliflower, bell peppers, green beans, aubergine, radish, cucumber, tomato etc.
– Increase antioxidant rich foods to reduce inflammation (which can drive insulin resistance), such as green tea, blueberries, blackberries, pomegranate, cherries, oily fish such as wild salmon, tomato puree, extra virgin olive oil, turmeric, ginger.
– Exercise promotes insulin sensitivity by improving uptake of glucose into skeletal muscle cells. Regular aerobic exercises and resistance training has been shown to be the most effective.
– Some nutritional deficiencies have been associated with insulin resistance, and optimising these levels could prove to be very helpful.
Magnesium, vitamin D, alpha lipoic acid, berberine and omega 3 fatty acids are some of the most extensively studied nutrients in insulin resistance (and type 2 diabetes).
Nutrition and lifestyle factors are the main determinants of good insulin sensitivity.
There isn’t a supplement that can compensate for a ‘bad’ diet or that can eliminate all the effects of stress.
High insulin, men, and fertility
In males, insulin surges increase conversion of testosterone to oestrogen (by a process called aromatisation).
This in turn throws off the oestrogen to testosterone ratio.
High aromatisation, resulting in high oestrogen, causes a binding protein, called Sex Hormone Binding Protein (SHBG) to increase.
This protein binds to oestrogen and testosterone thereby reducing the amount of ‘free’ testosterone i.e. the amount of ‘functional’ testosterone that is available.
As you can see, insulin can be a strong driver for a low amount of functional testosterone in men, and this is not great for fertility.
Testosterone replacement (gels or creams for example), can be devasting to male fertility.
Taking exogenous testosterone (that comes from outside of the body) switches off the pituitary hormones, as the body senses there is sufficient (or too much) testosterone.
Taking testosterone not produced by the body can suppress the body’s own signals to trigger testosterone production! (38)
And this isn’t always reversible when testosterone replacement is stopped.
High insulin can reduce testosterone.
A side effect of testosterone treatment is infertility.
Polycystic Ovary Syndrome (PCOS) in fertility
PCOS is a condition associated with higher levels of androgens.
Commonly, androgens are considered to be male hormones.
However, they are actually a group of sex hormones made in males and females, but in different amounts in each sex.
Men generally make more androgen hormones than women.
This group of sex hormones help to start puberty and play a role in reproductive health and body development.
Testosterone is the most common androgen.
In women, androgens can cause more follicles to develop in the ovaries.
But this is not healthy growth, and makes fertility more difficult to manage, even in an IVF setting.
One of the key drivers for the increased androgen levels in PCOS, is insulin.
The only meaningful way to manage insulin resistance is through nutrition and lifestyle interventions.
As you can see, a number of body systems are interlinked, and this is fundamental to the functional medicine approach to fertility (and many other health challenges!).
And in cases where there is a strong hereditary association with insulin resistance or type 2 diabetes, then supplemental support can be particularly effective in our experience.
PCOS can present itself in different ways.

It doesn’t have to present in the classical pearl-like cyst formation on ovaries that can be seen on an ultrasound.
High androgens alone can suggest PCOS.
Since PCOS is also associated with inflammation (39), the syndrome can affect ovarian reserve (the number and quality of eggs) and egg implantation.
Consistent nutritional and lifestyle interventions can help to turn the hormonal and metabolic (blood sugar regulation) changes around, and thereby improve both natural fertility and IVF success rates.
Optimising gut health can also positively influence PCOS – a healthy microbiome can improve insulin, inflammation, and hormonal changes.
Polycystic Ovary Syndrome can be modulated by addressing the drivers – such as insulin, inflammation, microbiome, diet, lifestyle, and stress.
The immune system link to fertility
The immune system comprises of a complex and extensive network of cells.
These cells, through communication with each other, and through the detection of ‘danger’ signals (originating from inside or outside of the body), produce a response that manifests as a symptom.
Perhaps more problematically, often the immune system does not create an obvious symptom, or is silent to us, so we don’t know there is an immune system problem.
We find that our clinical practice, in a good percentage of more complex infertility cases, there is an immune related imbalance.
In many cases, this could be THE cause of fertility issues.
What we’re really considering here, is a long term (chronic) immune response, rather than a short term immune response (e.g. the knee swelling) in response to an injury, where the immune response is supporting recovery.
So, what could our immune cells be reacting to, that it isn’t happy with?
- infections
- microbiome changes
- chemical or environmental toxins
- foods / drinks e.g. sensitivities to dairy or an allergy to peanut, or high alcohol, sugar or caffeine
- increased adipose tissue
- high oestrogen levels
- medications
- stress
- poor digestion
- poor liver detoxification
- chronic pain e.g. back pain
If the immune system is producing an inflammatory response, then it’s very relevant to fertility.
The immune system can be responding in different ways:
Inflammatory cytokines are molecules that drive inflammation and can damage cells and cellular functions.
Oxidative stress is when there is too many reactive oxygen species (ROS) and not enough antioxidants, and is a major contributing factor to egg and sperm quality, DNA stability and endometrial function.
Natural Killer (NK) cells are a type of white blood cell that protects us from ‘foreign’ threat, e.g. a virus, and has the ability to destroy these threats. NK cells are found in different regions of the body and in the blood.
They are also found in the uterus.
Uterine NK cells have received a considerable amount of attention in the fertility field due to their role in normal implantation and early placental development.
There is also a lot of controversy in NK cell testing, particularly around blood NK cell testing versus uterine NK cell testing.
The general consensus among experts is that uterine NK cells may be elevated even when blood levels are normal.
This means that testing blood NK levels may not be the best option when identifying whether NK cells are a problem.
High uterine NK cells are associated with increased inflammation and could be a cause of fertility problems (implantation failure or early pregnancy loss).
Other processes in chronic inflammation (that we won’t go into detail here) can include:
- CRP (C-reactive protein)
- ESR (Erythrocyte sedimentation rate)
- IgE (Immunoglobulin E)
- NF-Kb (Nuclear factor kappa B)
- TNF-a (Tumour necrosis factor α)
Autoimmunity in fertility
Autoimmune diseases are the result of the immune system mistakenly attacking the body (particular cell types, tissues or proteins for example).
For all autoimmune conditions, a Functional Medicine approach to fertility would be to:
– optimise the function of body systems, for example gastrointestinal, detoxification, endocrine (hormones) systems and ‘modulate’ the function of the immune system
– identify and address any infections, for example bacterial infections (e.g., helicobacter pylori, klebsiella, chlamydia pneumoniae, mycoplasma), yeast overgrowth such as candida albicans, or chronic viral infections (e.g., Epstein bar virus, herpes simplex and cytomegalovirus)
– identify and address any food allergies or sensitivities
– reduce exposure to, and eliminate as much as possible, any environmental chemicals
– reduce stress
– support a healthy lifestyle and immune modulation
Each of these areas would be assessed on an individual, personal basis.
The presence of autoimmune conditions in general can make it more difficult to conceive and maintain pregnancy.
However, there are some specific autoimmune conditions that should be explored in unexplained infertility.
Antiphospholipid Syndrome
Antiphospholipid Syndrome (APS) is an autoimmune condition which is 3 to 5 times more common in women than men.
In APS, the immune system produces antibodies to phospholipids (types of lipids, or fats) and increases risk of blood clots.
The condition can be a common cause of recurrent miscarriages.
Some estimate that APS accounts for 15% of cases of recurrent miscarriages (‘recurrent’ being medically defined, as three or more).
In our experience, it is not uncommon to find that the tests for antiphospholipid antibodies have not been performed in recurrent pregnancy loss cases.
Yet in some cases it is relatively straight forward to treat with anticoagulant (blood thinning) medications.
The antiphospholipid antibodies tested are:
- Lupus anticoagulant (LA) antibody
- Anticardiolipin (aCL) antibody
- Anti-b2-glycoprotein I antibody
Anti-sperm antibodies
Anti-sperm antibodies (ASA), first reported In 1954, can be produced in men (found in semen) or women (found in vaginal fluid) (40).
These antibodies can bind to sperm causing fertility issues, even when there are normal sperm parameters.
Anti-sperm antibody testing can often easily be added on when a semen analysis is being performed.
Studies have confirmed that by a process of molecular mimicry toward the bacteria Escherichia coli (E. coli), ASA can cause male infertility (41).
This means that a bacterial infection can be a causative factor in ASA generation and therefore infertility in men.
Research seems to be inconclusive for this causal relationship in women.
There are likely many other causal factors for ASA.
Thyroid antibodies in fertility
Thyroid antibodies should be assessed in all women with fertility issues (as we mentioned earlier).
Thyroid antibodies are:
- thyroid peroxidase
- thyroglobulin antibodies
Autoimmune thyroid disease is common in women, and low levels of antibodies during pregnancy is a risk factor for developing post-partum Hashimoto’s disease (autoimmune hypothyroidism).
Nutrition and lifestyle modifications may help to improve the picture.
One example of this is selenium supplementation.
Selenium has been shown to reduce thyroid antibody levels and improve thyroid function (42).
Environmental chemicals and pollutants
Environmental chemicals and pollutants are of great interest in a functional medicine approach to fertility.
The negative effects of chemicals and pollutants have been extensively studied.
Increased exposure to, or reduced detoxification of, environmental chemicals and pollutants, negatively affects both male and female fertility (and birth outcomes).
Some everyday chemicals such as:
- phthalates (plastics)
- pesticides
- dioxins
- air pollution
- triclosan
- parabens
- growth hormones in animal produce
- and chemicals in cosmetics
can act as ‘hormone disrupters’ (43).
Hormone disruptors exert their negative effects by acting on the hormone receptors in our body and disrupting normal hormone signalling.
The average person is exposed to endocrine disrupters on a daily basis due their ubiquitous presence in the environment.
The harmful effects of BPA (commonly found in plastic products) such as plastic bottles, was noted by the National Institute of Health (NIH) in 2008.
The NIH stated that BPA likely poses a risk to human development, and increases cancer risk.
Exposure to BPA early on in life has also been associated with the development of behavioural issues.
Industry has made significant progress in eliminating BPA from plastic bottles for example.
However, there are approximately 20 other types of plastics that are believed to be problematic, but which have not received anywhere near the same level of interest as BPA.
Going plastic-free is the best solution.
Experimental studies have also shown that phthalates can:
- disrupt follicle growth
- increase oxidative stress
- and cause a faster depletion of ovarian reserve (44)
Significantly higher levels of phthalates have been found in semen samples and urine samples from men with infertility (45).
Increased phthalate exposure can be associated with reduced morphology, sperm count and motility.
Hormone dysregulation caused by chemicals can also be a risk factor in hormone related conditions such as endometriosis, fibroids, and PCOS, which all affect fertility.
These synthetic chemicals can result in increased oxidative stress and inflammation.
In turn, this can:
- increase pro-inflammatory molecules in the peritoneal fluid
- injure testicular Leydig and Sertoli cells (which produce testosterone and sperm cells, respectively)
- reduce ovarian count / reserve
- and promote autoimmunity

Studies have shown that air pollution on its own can increase rate of infertility, through causing increased oxidative stress (46).
Environmental chemicals have an effect on multiple pathways in the body.
They can cause:
- inflammation (47)
- endocrine disruption (48)
- oxidative stress (49)
- interference with normal DNA methylation processes (processes that keep DNA stable) (50)
- the minimisation of epigenetic changes (changes to how your body reads DNA, without there actually being a change to the DNA sequence, which can also be inheritable changes) (50)
This can affect not only conception rate, IVF success, and pregnancy duration, but can also affect the offspring.
Genetically, some men and women may be at greater risk of chemicals and pollutants than others, due to reduced expression of detoxification enzymes.
Reduced detoxification increases the levels of chemicals and pollutants in the body, potentially causing more harm compared to those who detoxify efficiently.
Through advanced testing we can gain insight into the functioning of these detoxification pathways.
Testing options include genetic based tests to assess if one gene may be producing too low levels of enzymes that support detoxification (for example the GST, CYP1, CYP1, CYP2, CYP3, COMT, NAT and SOD genes).
Or genetic based tests may offer signs that increased support is required in certain detoxification pathways, through measuring levels of pyroglutamate, alpha-hydroxybutyrate and glucarate, for example.
Assessing how oestrogen is being metabolised in the liver can also provide important clues about liver detoxification processes. An ‘environmental clean-up’ is essential (even if there are no fertility issues, as toxin chemicals can also impact the baby) (51, 52).
We recommend to:
- eliminate all plastics
- replace plastic water bottles with glass or stainless steel bottles (even if the bottle is ‘BPA free’)
- take the plastic lid off the coffee container before drinking it
- eliminate cling film
- use other non-plastic food storage solutions
Replacing all household products and cosmetics with natural, chemical free products, can have a tremendous positive impact to your health, fertility and the health of the next two generations of children.
We now know that health in-utero (before birth) can affect the health, and disease risk, of not only the offspring, but in their children also, through epigenetic changes (53).
As you can see, environmental chemicals should always be considered in a functional medicine approach to fertility.
Methylation in fertility
Methylation is a cellular process whereby a methyl group (one carbon and three hydrogen molecules) is donated from one substance to another and this transfer of methyl groups helps to drive certain reactions.
Methylation has a role to play in areas such as:
- DNA stability
- epigenetic changes
- detoxification
- neurotransmitter synthesis
- cancer risk
- fertility
- and mood
Some experts have estimated that approximately 40% of humans may not be methylating optimally, due to our genetics.
The most studied genetic variance concerning methylation, is the MTHFR gene (which encodes for the methyl tetra hydrofolate reductase enzyme), at gene locations A1298 and C677.
Methylating genes are one of several factors we often like to test for through a fertility related genetic test.
Through appropriate dietary and nutritional support, methylation can be supported.
Please note, though, that over supplementing to support methylation can lead to hyper-methylation, which is just as problematic as hypo-methylating).
Optimal methylation supports fertility and can reduce early pregnancy loss risk.
Ensuring a diet is rich in vitamins B2, B6, B9 (folate), B12, betaine and magnesium can support methylation.
Body composition, body fat percentage, and fertility
A healthy body fat percentage for men and women is an important determinant of hormone signalling.
Either too high or too of a low body fat percentage can be an issue.
Low body fat (or low BMI) in women can cause disturbances to the pituitary hormones, leading to irregular cycles, lack of ovulation or amenorrhea (absence of periods) (54).
Some body fat is required to help regulate hormones and synthesise healthy levels of oestrogen.
In overweight women, (defined as high body fat or high BMI (when there isn’t a high amount of muscle mass)), being overweight can impair the development of the egg (55) and reduce endometrial receptivity (56).
In cases where there is also insulin resistance, then an increase in androgens could result in anovulation (when an egg doesn’t release from the ovary) and low progesterone levels.
It is widely held that even moderate weight loss can usually reverse these fertility issues.
In men, obesity can impair sperm production and cause damage in sperm DNA (increased DNA fragmentation) which is a significant factor in conception rates and miscarriages (57).
Too low a BMI or body fat percentage in men can cause reduced testosterone levels.
A tailored nutritional protocol can help achieve optimal body weight / fat percentage to support fertility.
Apply for your free 15 minute Discovery Call with Dee Brereton-Patel now
The wrap: the natural approach to fertility is complex!
Wow! That was a really long and complex article wasn’t it?!
We understand that the fertility journey can be really challenging, really frustrating, and really emotionally draining.
Here are a few conclusions that we’ve reached over our years of working with hundreds of fertility clients, conclusions that you might have reached too:
– with the number of systems and factors involved, fertility and infertility can be a really complex and highly personalised journey
– if you’re having trouble conceiving, are thinking of going down the IVF route, or are considering surrogacy, there’s a lot that can be done to optimise your journey and increase your chances of success
– ‘going it alone’ and trying to work it out yourself is difficult and can lead to years of frustration, heart-ache or wasted rounds of IVF treatment
If you think a natural, Functional Medicine approach to fertility can help you, you can book a free 15 minute discovery call with us here.
To your healthier future,
Dee & the Coho Health team

How can we help you? Send us a message below and we’ll come right back to you…
1.
Agarwal A, Mulgund A, Hamada A, Chyatte MR. A unique view on male infertility around the globe. Reprod Biol Endocrinol. 2015 Apr 26;13:37. doi: 10.1186/s12958-015-0032-1. PMID: 25928197; PMCID: PMC4424520
2.
Wang D, Jiang Y, Feng J, Gao J, Yu J, Zhao J, Liu P, Han Y. Evidence for the Use of Complementary and Alternative Medicine for Pelvic Inflammatory Disease: A Literature Review. Evid Based Complement Alternat Med. 2022 Jan 19;2022:1364297. doi: 10.1155/2022/1364297. PMID: 35096102; PMCID: PMC8791705.
3.
Khalaf Y. ABC of subfertility. Tubal subfertility. BMJ. 2003 Sep 13;327(7415):610-3. doi: 10.1136/bmj.327.7415.610. PMID: 12969933; PMCID: PMC194096.
4.
Simon A, Laufer N. Assessment and treatment of repeated implantation failure (RIF). J Assist Reprod Genet. 2012 Nov;29(11):1227-39. doi: 10.1007/s10815-012-9861-4. Epub 2012 Sep 14. PMID: 22976427; PMCID: PMC3510376.
5.
Hosseinirad H, Yadegari P, Falahieh FM, Shahrestanaki JK, Karimi B, Afsharzadeh N, Sadeghi Y. The impact of congenital uterine abnormalities on pregnancy and fertility: a literature review. JBRA Assist Reprod. 2021 Oct 4;25(4):608-616. doi: 10.5935/1518-0557.20210021. PMID: 34224238; PMCID: PMC8489822.
6.
Bani Mohammad M, Majdi Seghinsara A. Polycystic Ovary Syndrome (PCOS), Diagnostic Criteria, and AMH. Asian Pac J Cancer Prev. 2017 Jan 1;18(1):17-21. doi: 10.22034/APJCP.2017.18.1.17. PMID: 28240001; PMCID: PMC5563096.
7.
Bulletti C, Coccia ME, Battistoni S, Borini A. Endometriosis and infertility. J Assist Reprod Genet. 2010 Aug;27(8):441-7. doi: 10.1007/s10815-010-9436-1. Epub 2010 Jun 25. PMID: 20574791; PMCID: PMC2941592.
8.
Jin L, Ruan X, Jin J, Wang Y, Zhang Y, Zhou Q, Lu D, Mueck AO. Infertile women with endometriosis possess differences in cytokine levels in various tissues. Gynecol Endocrinol. 2022 Jun;38(6):523-527. doi: 10.1080/09513590.2022.2060961. Epub 2022 Apr 9. PMID: 35403529.
9.
Guo XC, Segars JH. The impact and management of fibroids for fertility: an evidence-based approach. Obstet Gynecol Clin North Am. 2012 Dec;39(4):521-33. doi: 10.1016/j.ogc.2012.09.005. PMID: 23182558; PMCID: PMC3608270.
10.
Weiss G, Goldsmith LT, Taylor RN, Bellet D, Taylor HS. Inflammation in reproductive disorders. Reprod Sci. 2009 Feb;16(2):216-29. doi: 10.1177/1933719108330087. PMID: 19208790; PMCID: PMC3107847.
11.
Kupis Ł, Dobroński PA, Radziszewski P. Varicocele as a source of male infertility – current treatment techniques. Cent European J Urol. 2015;68(3):365-70. doi: 10.5173/ceju.2015.642. Epub 2015 Oct 15. PMID: 26568883; PMCID: PMC4643713.
12.
Kantartzi PD, Goulis ChD, Goulis GD, Papadimas I. Male infertility and varicocele: myths and reality. Hippokratia. 2007 Jul;11(3):99-104. PMID: 19582201; PMCID: PMC2658802
13.
Lavranos G, Balla M, Tzortzopoulou A, Syriou V, Angelopoulou R. Investigating ROS sources in male infertility: a common end for numerous pathways. Reprod Toxicol. 2012 Nov;34(3):298-307. doi: 10.1016/j.reprotox.2012.06.007. Epub 2012 Jun 28. PMID: 22749934.
14.
Jefferys A, Siassakos D, Wardle P. The management of retrograde ejaculation: a systematic review and update. Fertil Steril. 2012 Feb;97(2):306-12. doi: 10.1016/j.fertnstert.2011.11.019. Epub 2011 Dec 15. PMID: 22177462.
15.
Mesen TB, Young SL. Progesterone and the luteal phase: a requisite to reproduction. Obstet Gynecol Clin North Am. 2015 Mar;42(1):135-51. doi: 10.1016/j.ogc.2014.10.003. Epub 2015 Jan 5. PMID: 25681845; PMCID: PMC4436586.
16.
Healy DL, Schenken RS, Lynch A, Williams RF, Hodgen GD. Pulsatile progesterone secretion: its relevance to clinical evaluation of corpus luteum function. Fertil Steril. 1984 Jan;41(1):114-21. doi: 10.1016/s0015-0282(16)47551-5. PMID: 6537924.
17.
Marquardt RM, Kim TH, Shin JH, Jeong JW. Progesterone and Estrogen Signaling in the Endometrium: What Goes Wrong in Endometriosis? Int J Mol Sci. 2019 Aug 5;20(15):3822. doi: 10.3390/ijms20153822. PMID: 31387263; PMCID: PMC6695957.
18.
Kwa M, Plottel CS, Blaser MJ, Adams S. The Intestinal Microbiome and Estrogen Receptor-Positive Female Breast Cancer. J Natl Cancer Inst. 2016 Apr 22;108(8):djw029. doi: 10.1093/jnci/djw029. PMID: 27107051; PMCID: PMC5017946.
19.
Grande G, Barrachina F, Soler-Ventura A, Jodar M, Mancini F, Marana R, Chiloiro S, Pontecorvi A, Oliva R, Milardi D. The Role of Testosterone in Spermatogenesis: Lessons From Proteome Profiling of Human Spermatozoa in Testosterone Deficiency. Front Endocrinol (Lausanne). 2022 May 19;13:852661. doi: 10.3389/fendo.2022.852661. PMID: 35663320; PMCID: PMC9161277.
20.
Nedresky D, Singh G. Physiology, Luteinizing Hormone. 2021 Sep 28. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan–. PMID: 30969514.
21.
Gollenberg AL, Liu F, Brazil C, Drobnis EZ, Guzick D, Overstreet JW, Redmon JB, Sparks A, Wang C, Swan SH. Semen quality in fertile men in relation to psychosocial stress. Fertil Steril. 2010 Mar 1;93(4):1104-11. doi: 10.1016/j.fertnstert.2008.12.018. Epub 2009 Feb 24. PMID: 19243749.
22.
Frederiksen Y, Farver-Vestergaard I, Skovgård NG, Ingerslev HJ, Zachariae R. Efficacy of psychosocial interventions for psychological and pregnancy outcomes in infertile women and men: a systematic review and meta-analysis. BMJ Open. 2015 Jan 28;5(1):e006592. doi: 10.1136/bmjopen-2014-006592. PMID: 25631310; PMCID: PMC4316425.
23.
Poppe K, Bisschop P, Fugazzola L, Minziori G, Unuane D, Weghofer A. 2021 European Thyroid Association Guideline on Thyroid Disorders prior to and during Assisted Reproduction. Eur Thyroid J. 2021 Feb;9(6):281-295. doi: 10.1159/000512790. Epub 2021 Jan 21. Erratum in: Eur Thyroid J. 2021 Jun;10(3):268. PMID: 33718252; PMCID: PMC7923920.
24.
Negro R, Schwartz A, Gismondi R, Tinelli A, Mangieri T, Stagnaro-Green A. Increased pregnancy loss rate in thyroid antibody negative women with TSH levels between 2.5 and 5.0 in the first trimester of pregnancy. J Clin Endocrinol Metab. 2010 Sep;95(9):E44-8. doi: 10.1210/jc.2010-0340. Epub 2010 Jun 9. PMID: 20534758.
25.
Akhtar MA, Agrawal R, Brown J, Sajjad Y, Craciunas L. Thyroxine replacement for subfertile women with euthyroid autoimmune thyroid disease or subclinical hypothyroidism. Cochrane Database Syst Rev. 2019 Jun 25;6(6):CD011009. doi: 10.1002/14651858.CD011009.pub2. PMID: 31236916; PMCID: PMC6591496
26.
Deroux A, Dumestre-Perard C, Dunand-Faure C, Bouillet L, Hoffmann P. Female Infertility and Serum Auto-antibodies: a Systematic Review. Clin Rev Allergy Immunol. 2017 Aug;53(1):78-86. doi: 10.1007/s12016-016-8586-z. PMID: 27628237.
27.
Zhong YP, Ying Y, Wu HT, Zhou CQ, Xu YW, Wang Q, Li J, Shen XT, Li J. Relationship between antithyroid antibody and pregnancy outcome following in vitro fertilization and embryo transfer. Int J Med Sci. 2012;9(2):121-5. doi: 10.7150/ijms.3467. Epub 2012 Jan 5. PMID: 22253557; PMCID: PMC3258552.
28.
Sengupta P, Dutta S, Karkada IR, Chinni SV. Endocrinopathies and Male Infertility. Life (Basel). 2021 Dec 22;12(1):10. doi: 10.3390/life12010010. PMID: 35054403; PMCID: PMC8779600.
29.
Kaiser UB. Hyperprolactinemia and infertility: new insights. J Clin Invest. 2012 Oct;122(10):3467-8. doi: 10.1172/jci64455. PMID: 23193578; PMCID: PMC3461927.
30.
Singh P, Singh M, Cugati G, Singh AK. Hyperprolactinemia: An often missed cause of male infertility. J Hum Reprod Sci. 2011 May;4(2):102-3. doi: 10.4103/0974-1208.86094. PMID: 22065670; PMCID: PMC3205532.
31.
Shimobayashi M, Albert V, Woelnerhanssen B, Frei IC, Weissenberger D, Meyer-Gerspach AC, Clement N, Moes S, Colombi M, Meier JA, Swierczynska MM, Jenö P, Beglinger C, Peterli R, Hall MN. Insulin resistance causes inflammation in adipose tissue. J Clin Invest. 2018 Apr 2;128(4):1538-1550. doi: 10.1172/JCI96139. Epub 2018 Mar 12. PMID: 29528335; PMCID: PMC5873875.
32.
Asmat U, Abad K, Ismail K. Diabetes mellitus and oxidative stress-A concise review. Saudi Pharm J. 2016 Sep;24(5):547-553. doi: 10.1016/j.jsps.2015.03.013. Epub 2015 Mar 21. PMID: 27752226; PMCID: PMC5059829.
33.
Guo S. Insulin signaling, resistance, and the metabolic syndrome: insights from mouse models into disease mechanisms. J Endocrinol. 2014 Jan 8;220(2):T1-T23. doi: 10.1530/JOE-13-0327. PMID: 24281010; PMCID: PMC4087161.
34.
Mansour R, El-Faissal Y, Kamel A, Kamal O, Aboulserour G, Aboulghar M, Fahmy I. Increased insulin resistance in men with unexplained infertility. Reprod Biomed Online. 2017 Nov;35(5):571-575. doi: 10.1016/j.rbmo.2017.08.020. Epub 2017 Aug 24. PMID: 28888863.
35.
Wang H, Zhang Y, Fang X, Kwak-Kim J, Wu L. Insulin Resistance Adversely Affect IVF Outcomes in Lean Women Without PCOS. Front Endocrinol (Lausanne). 2021 Sep 6;12:734638. doi: 10.3389/fendo.2021.734638. PMID: 34552564; PMCID: PMC8450607.
36.
Unluhizarci K, Karaca Z, Kelestimur F. Role of insulin and insulin resistance in androgen excess disorders. World J Diabetes. 2021 May 15;12(5):616-629. doi: 10.4239/wjd.v12.i5.616. PMID: 33995849; PMCID: PMC8107978.
37.
Werdermann M, Berger I, Scriba LD, Santambrogio A, Schlinkert P, Brendel H, Morawietz H, Schedl A, Peitzsch M, King AJF, Andoniadou CL, Bornstein SR, Steenblock C. Insulin and obesity transform hypothalamic-pituitary-adrenal axis stemness and function in a hyperactive state. Mol Metab. 2021 Jan;43:101112. doi: 10.1016/j.molmet.2020.101112. Epub 2020 Nov 4. PMID: 33157254; PMCID: PMC7691554.
38.
Sukegawa G, Tsuji Y. [Risk of Male Infertility Due to Testosterone Replacement Therapy for Late-Onset Hypogonadism (LOH)]. Hinyokika Kiyo. 2020 Nov;66(11):407-409. Japanese. doi: 10.14989/ActaUrolJap_66_11_407. PMID: 33271659.
39.
Duleba AJ, Dokras A. Is PCOS an inflammatory process? Fertil Steril. 2012 Jan;97(1):7-12. doi: 10.1016/j.fertnstert.2011.11.023. PMID: 22192135; PMCID: PMC3245829.
40.
A S V, Dhama K, Chakraborty S, Samad HA, Latheef SK, Sharun K, Khurana SK, K A, Tiwari R, Bhatt P, K V, Chaicumpa W. Role of Antisperm Antibodies in Infertility, Pregnancy, and Potential forContraceptive and Antifertility Vaccine Designs: Research Progress and Pioneering Vision. Vaccines (Basel). 2019 Sep 16;7(3):116. doi: 10.3390/vaccines7030116. PMID: 31527552; PMCID: PMC6789593.
41.
Thaper D, Prabha V. Molecular mimicry: An explanation for autoimmune diseases and infertility. Scand J Immunol. 2018 Jun 23:e12697. doi: 10.1111/sji.12697. Epub ahead of print. PMID: 29935034.
42.
Zuo Y, Li Y, Gu X, Lei Z. The correlation between selenium levels and autoimmune thyroid disease: a systematic review and meta-analysis. Ann Palliat Med. 2021 Apr;10(4):4398-4408. doi: 10.21037/apm-21-449. Epub 2021 Apr 16. PMID: 33894732.
43.
Chiang C, Mahalingam S, Flaws JA. Environmental Contaminants Affecting Fertility and Somatic Health. Semin Reprod Med. 2017 May;35(3):241-249. doi: 10.1055/s-0037-1603569. Epub 2017 Jun 28. PMID: 28658707; PMCID: PMC6425478.
44.
Panagiotou EM, Ojasalo V, Damdimopoulou P. Phthalates, ovarian function and fertility in adulthood. Best Pract Res Clin Endocrinol Metab. 2021 Sep;35(5):101552. doi: 10.1016/j.beem.2021.101552. Epub 2021 Jun 2. PMID: 34238683.
45.
Radke EG, Braun JM, Meeker JD, Cooper GS. Phthalate exposure and male reproductive outcomes: A systematic review of the human epidemiological evidence. Environ Int. 2018 Dec;121(Pt 1):764-793. doi: 10.1016/j.envint.2018.07.029. Epub 2018 Oct 16. Erratum in: Environ Int. 2019 Apr;125:606-607. PMID: 30336412.
46.
Conforti A, Mascia M, Cioffi G, De Angelis C, Coppola G, De Rosa P, Pivonello R, Alviggi C, De Placido G. Air pollution and female fertility: a systematic review of literature. Reprod Biol Endocrinol. 2018 Dec 30;16(1):117. doi: 10.1186/s12958-018-0433-z. PMID: 30594197; PMCID: PMC6311303.
47.
Vitti M, Di Emidio G, Di Carlo M, Carta G, Antonosante A, Artini PG, Cimini A, Tatone C, Benedetti E. Peroxisome Proliferator-Activated Receptors in Female Reproduction and Fertility. PPAR Res. 2016;2016:4612306. doi: 10.1155/2016/4612306. Epub 2016 Jul 31. PMID: 27559343; PMCID: PMC4983391.
48.
Gonsioroski A, Mourikes VE, Flaws JA. Endocrine Disruptors in Water and Their Effects on the Reproductive System. Int J Mol Sci. 2020 Mar 12;21(6):1929. doi: 10.3390/ijms21061929. PMID: 32178293; PMCID: PMC7139484.
49.
Al-Gubory KH. Environmental pollutants and lifestyle factors induce oxidative stress and poor prenatal development. Reprod Biomed Online. 2014 Jul;29(1):17-31. doi: 10.1016/j.rbmo.2014.03.002. Epub 2014 Mar 21. PMID: 24813750.
50.
Singh S, Li SS. Epigenetic effects of environmental chemicals bisphenol A and phthalates. Int J Mol Sci. 2012;13(8):10143-53. doi: 10.3390/ijms130810143. Epub 2012 Aug 15. PMID: 22949852; PMCID: PMC3431850.
51.
Smith LE, Prendergast AJ, Turner PC, Humphrey JH, Stoltzfus RJ. Aflatoxin Exposure During Pregnancy, Maternal Anemia, and Adverse Birth Outcomes. Am J Trop Med Hyg. 2017 Apr;96(4):770-776. doi: 10.4269/ajtmh.16-0730. PMID: 28500823; PMCID: PMC5392618.
52.
Padula AM, Monk C, Brennan PA, Borders A, Barrett ES, McEvoy CT, Foss S, Desai P, Alshawabkeh A, Wurth R, Salafia C, Fichorova R, Varshavsky J, Kress A, Woodruff TJ, Morello-Frosch R; program collaborators for Environmental influences on Child Health Outcomes. A review of maternal prenatal exposures to environmental chemicals and psychosocial stressors-implications for research on perinatal outcomes in the ECHO program. J Perinatol. 2020 Jan;40(1):10-24. doi: 10.1038/s41372-019-0510-y. Epub 2019 Oct 15. PMID: 31616048; PMCID: PMC6957228.
53.
Kaspar D, Hastreiter S, Irmler M, Hrabé de Angelis M, Beckers J. Nutrition and its role in epigenetic inheritance of obesity and diabetes across generations. Mamm Genome. 2020 Jun;31(5-6):119-133. doi: 10.1007/s00335-020-09839-z. Epub 2020 Apr 30. PMID: 32350605; PMCID: PMC7368866.
54.
Frisch RE. The right weight: body fat, menarche and ovulation. Baillieres Clin Obstet Gynaecol. 1990 Sep;4(3):419-39. doi: 10.1016/s0950-3552(05)80302-5. PMID: 2282736.
55.
Purcell SH, Moley KH. The impact of obesity on egg quality. J Assist Reprod Genet. 2011 Jun;28(6):517-24. doi: 10.1007/s10815-011-9592-y. Epub 2011 May 28. PMID: 21625966; PMCID: PMC3158259.
56.
Bellver J, Marín C, Lathi RB, Murugappan G, Labarta E, Vidal C, Giles J, Cabanillas S, Marzal A, Galliano D, Ruiz-Alonso M, Simón C, Valbuena D. Obesity Affects Endometrial Receptivity by Displacing the Window of Implantation. Reprod Sci. 2021 Nov;28(11):3171-3180. doi: 10.1007/s43032-021-00631-1. Epub 2021 May 25. PMID: 34033112.
57.
Campbell JM, Lane M, Owens JA, Bakos HW. Paternal obesity negatively affects male fertility and assisted reproduction outcomes: a systematic review and meta-analysis. Reprod Biomed Online. 2015 Nov;31(5):593-604. doi: 10.1016/j.rbmo.2015.07.012. Epub 2015 Aug 10. PMID: 26380863.